CASE 11 Chronic Total Occlusion Intervention
Cardiac catheterization
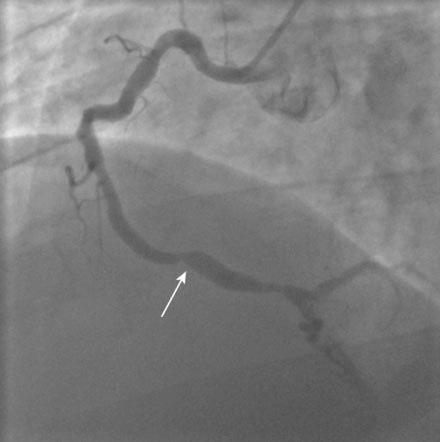
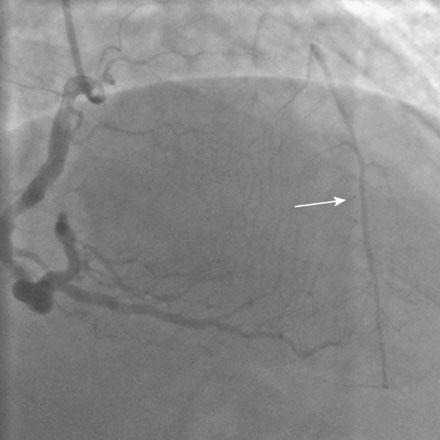
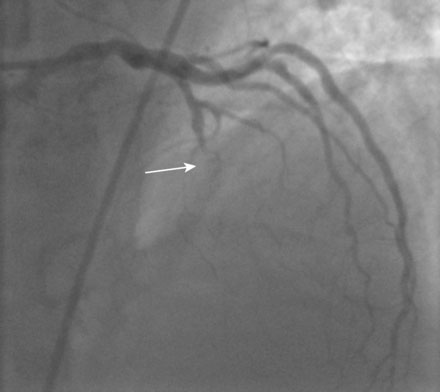
The left ventriculogram was normal, with an ejection fraction of 60% and no segmental wall motion abnormalities. A severe stenosis was noted in the right coronary artery (Figure 11-1). There was also a prominent collateral vessel to the left anterior descending (LAD) artery (Figure 11-2 and Video 11-1). As was suspected because of the presence of collateral circulation from the right coronary artery, there was total occlusion of the LAD. The circumflex artery appeared free of significant narrowing (Figures 11-3, 11-4 and Video 11-2). Although the right coronary lesion appeared readily amenable to percutaneous coronary intervention (PCI), the angiographic appearance and clinical history suggested that the LAD occlusion was likely chronic and might not be successfully treated percutaneously. The physician decided to terminate the procedure and discuss therapeutic options in more detail with the patient.

The patient returned to the cardiac catheterization laboratory. The operator decided to use the prominent collateral to the LAD from the right coronary artery to help guide attempts at crossing the occluded segment. Therefore, two angiographic manifolds were prepared and femoral arterial access obtained from both the right and left femoral arteries. After engaging the right coronary artery with a diagnostic catheter and the left coronary artery with a guide catheter, contrast was injected first in the right coronary artery and then in the left coronary to define the extent of the LAD occlusion (Figure 11-5 and Video 11-3).
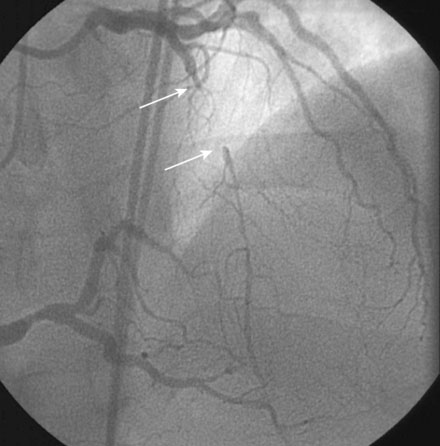
FIGURE 11-5 Simultaneous injection of the right and left coronary arteries shows the extent of the occlusion (arrows).
Unfractionated heparin was administered as a bolus to achieve a therapeutic activated clotting time; clopidogrel had not been given prior to the procedure in the event that PCI was unsuccessful and bypass surgery was required. The operator chose a tapered tip guidewire specifically designed for chronic total occlusions (Asahi Miracle Bros 3.0) and loaded this wire into a 2.0 mm diameter by 20 mm long “over-the-wire” compliant balloon. In the right anterior oblique projection, the operator advanced the stiff-tipped guidewire through the occluded segment, using occasional injections into the right coronary artery to visualize the collateral. Eventually, it appeared that the wire had advanced all the way through the occlusion (Figure 11-6 and Video 11-4). Angiography of the wire and collateral in the lateral projection, however, demonstrated that the wire tip was parallel to the artery and not in the true lumen of the LAD (Figure 11-7 and Video 11-5). The wire was gently withdrawn and repositioned, ultimately achieving the distal lumen of the LAD (Figure 11-8 and Video 11-6). The balloon easily advanced through the occlusion but, prior to inflation, the operator removed the guidewire and gently injected contrast through the balloon lumen to confirm location within the true lumen of the distal LAD (Figure 11-9 and Video 11-7). A floppy-tipped, 0.014 inch guidewire was reinserted within the balloon catheter and positioned distally in the LAD, and balloon angioplasty was performed with a 2.5 mm compliant balloon followed by placement of two sirolimus-eluting stents (2.5 mm diameter by 28 mm long stent distally and a 2.75 mm diameter by 13 mm long stent proximally). The final angiographic result for the LAD is shown in Figure 11-10
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


