CASE 10 PCI of an Ostial Right Coronary Artery Lesion
Cardiac catheterization
Coronary angiography found no significant obstructive disease in the left coronary artery (Figure 10-1) but a severe ostial stenosis of the right coronary artery, with extensive calcification (Figure 10-2 and Video 10-1). Based on the angiogram, her physician decided to proceed with a percutaneous approach and, anticipating great difficulty because of the ostial location and the degree of calcification observed, the operator planned to debulk the lesion with rotational atherectomy.

FIGURE 10-1 This is the left coronary angiogram; there were no significant obstructive lesions noted.

Femoral venous access was obtained and a temporary pacemaker wire positioned in the right ventricular apex. The operator then engaged an 8 French right Judkins guide catheter with side holes and administered eptifibatide as a double bolus plus infusion along with unfractionated heparin to achieve an activated clotting time (ACT) greater than 200 seconds. A floppy-tipped rotational atherectomy guidewire was positioned distally in the right coronary artery. Rotational atherectomy was accomplished first with a 1.5 mm burr, followed by a 2.0 mm burr. The angiographic result after rotational atherectomy is shown in Figure 10-3 and Video 10-2. The operator removed the rotational atherectomy guidewire and positioned a conventional 0.014 inch floppy-tipped guidewire distally in the right coronary artery. The lesion was dilated with a 3.0 mm diameter by 20 mm long compliant balloon and a 3.5 mm diameter by 23 mm long sirolimus-eluting stent positioned to cover the ostium (Figure 10-4 and Video 10-3) and postdilated with a 4.0 mm diameter by 9 mm long noncompliant balloon to high pressures. The final angiographic images satisfied the operator, although mild narrowing remained at the ostium (Figure 10-5 and Video 10-4); intravascular ultrasound was not performed and the procedure was terminated.


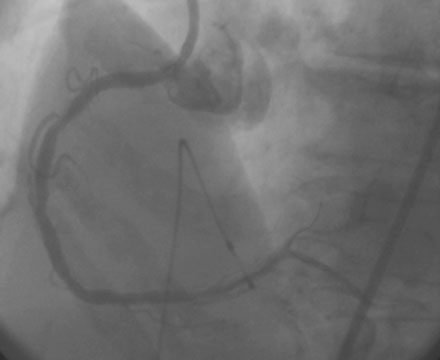
FIGURE 10-4 This figure demonstrates the position of the stent relative to the right coronary ostium.
Postprocedural course
She remained symptom-free for 5 months, and then developed recurrent severe chest pain similar to her initial symptoms. She was again admitted to the hospital, but this time, serial troponins were negative. Repeat cardiac catheterization revealed severe, in-stent restenosis of the ostium of the right coronary artery (Figure 10-6
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


