10: Chronic Thrombus and Metastatic Cancer—An Unexpected CTEPH Mimic
Figure 10.1
Computed tomographyof the chest demonstrating thickening of the wall of the left pulmonary artery (blue arrow), occlusive thrombus in the proximal right PA (solid white arrow) and vessel attenuation of the right lower lobe arteries (open white arrow)
Pulmonary function testing revealed an FEV1 of 81% predicted, and FVC of 94% predicted with an FEV1/FVC of 62%. The DLCO was decreased at 45% predicted. A TTE showed a left ventricular ejection fraction of 60–65%. The right ventricle was dilated with right ventricular hypertrophy and a moderate decrease in systolic function. The estimated pulmonary artery systolic pressure was 75–80 mmHg. A recent right heart catheterization demonstrated pulmonary hypertension. The right atrial pressure was 27 mmHg, the pulmonary artery pressure was 91/23(46) mmHg and the pulmonary capillary wedge pressure was 10 mmHg. The cardiac output by thermodilution was 4.2 L/min and the pulmonary vascular resistance was 8.5 Woods units. A ventilation perfusion scan showed multiple mismatched perfusion abnormalities (Fig. 10.2).
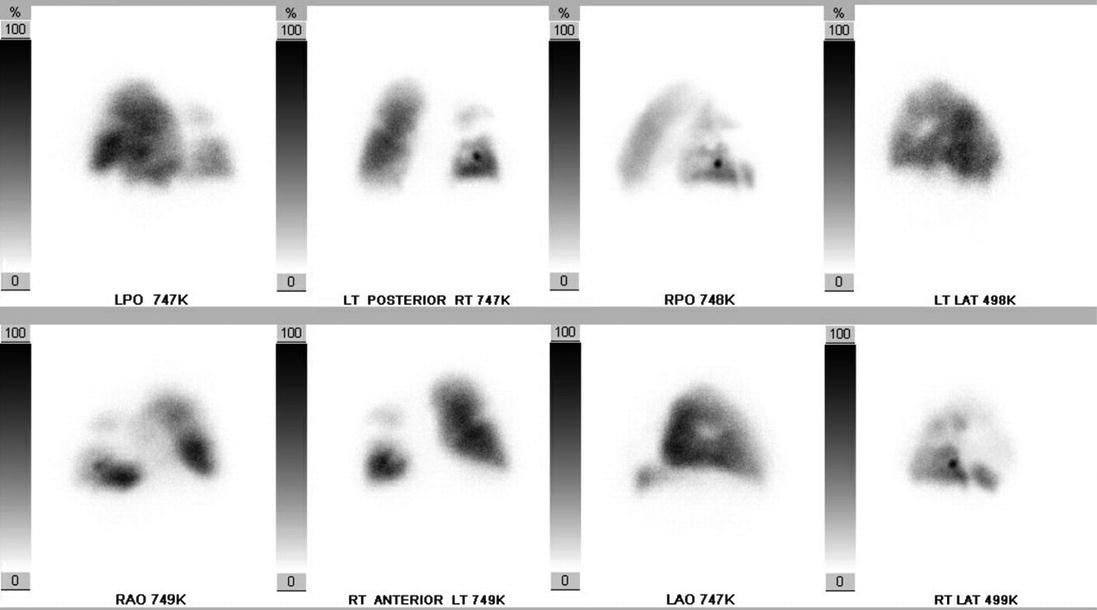
Figure 10.2
The ventilation-perfusion scan. The ventilation images were normal. The perfusion scan demonstrated multiple defects consistent with acute or chronic pulmonary embolism
The patient was diagnosed with chronic thromboembolic pulmonary hypertension and admitted to the hospital for further management.
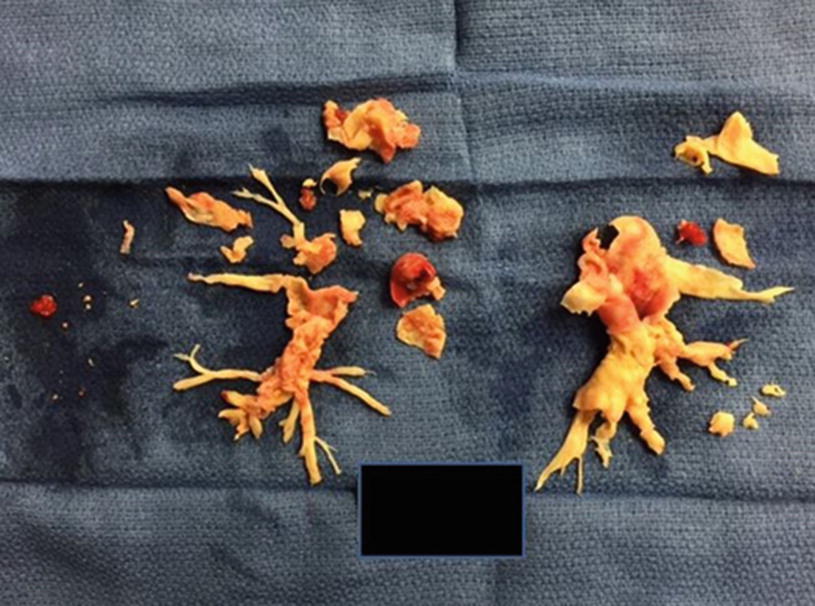
The patient was admitted to the hospital and treated with intravenous diuretics. Supplemental oxygen was used to maintain an oxygen saturation >95%. On day 4 of hospitalization she underwent pulmonary thromboendarterectomy (Fig. 10.3).
Figure 10.3
The endarterectomy specimen from the patient
Only gold members can continue reading. Log In or Register to continue