CASE 1 Restenosis of a Drug-Eluting Stent
Case presentation
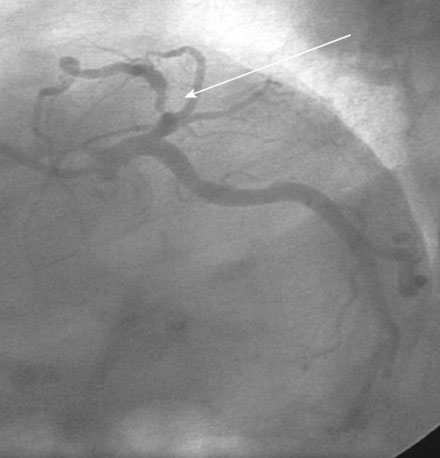
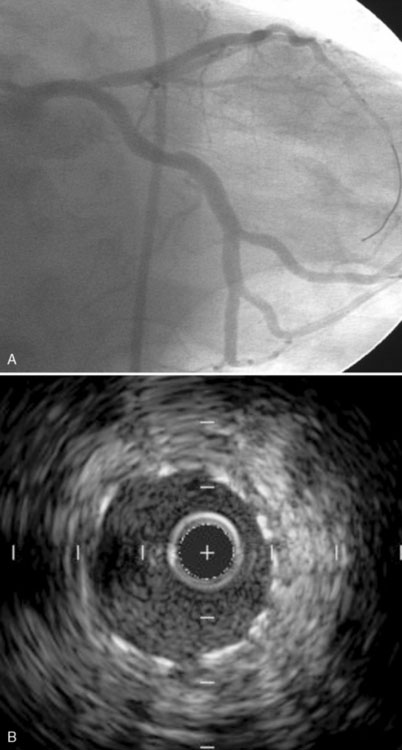
Two years earlier, he first developed classic effort angina. An abnormal stress test led to a coronary angiogram, which revealed a severe stenosis in the proximal segment of the left anterior descending coronary artery (Figure 1-1 and Video 1-1). This was treated with a 3.0 mm diameter by 23 mm long sirolimus-eluting stent, with an excellent angiographic result (Figure 1-2 and Video 1-2). His angina completely resolved; however, 10 months after the procedure, he developed recurrent effort angina. Coronary angiography confirmed severe, focal, in-stent restenosis within the proximal edge of the drug-eluting stent (Figure 1-3). Balloon angioplasty using a 3.0 mm noncompliant balloon dilated to 16 atmospheres improved the angiographic appearance (Figure 1-4 and Video 1-3) and resolved the patient’s symptoms. However, 6 months later (and 9 months before his current presentation) the development of recurrent angina prompted another angiogram. A second recurrence of in-stent restenosis within the proximal left anterior descending artery stent (Figure 1-5 and Video 1-4) was treated with a 3.0 mm diameter by 30 mm long zotarolimus-eluting stent, again with good angiographic result (Figure 1-6A). Intravascular ultrasound performed after this procedure demonstrated excellent stent apposition throughout the stented segment (Figure 1-6B). He remained symptom-free for 6 months until this presentation.
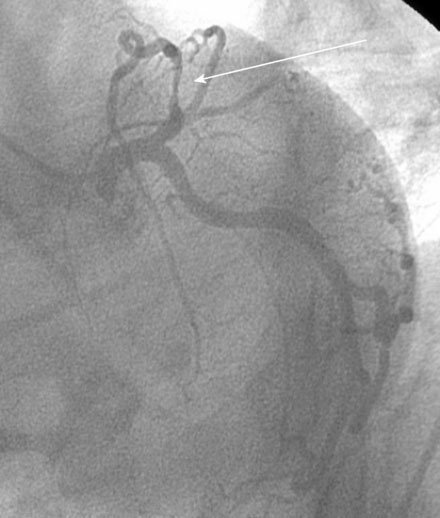

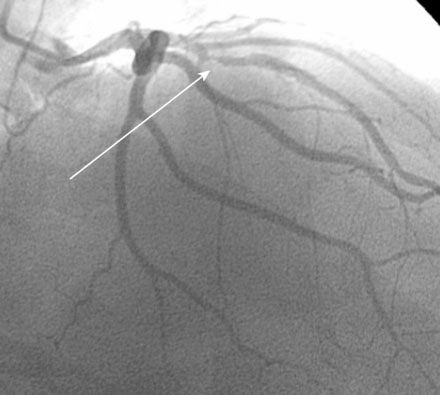
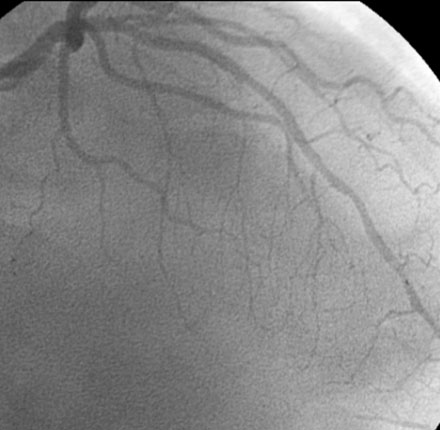
FIGURE 1-4 This is the result after balloon angioplasty of the restenotic lesion in the proximal left anterior descending artery shown in Figure 1-3.