Anatomy
Thorax
Before describing the anatomy of the heart, it is helpful to review other anatomic features of the thoracic cavity and organs.
The thorax proper constitutes the upper part of the body or trunk, with a shape between a barrel and a truncated cone that is functionally favorable. Although the intrathoracic pressure is often subatmospheric, the chest wall is still able to retain its integrity by means of rather thin, lightweight skeletal elements. The thoracic cavity occupies only the upper part of the thoracic cage. The abdominal (peritoneal) cavity reaches upward as high as the lower tip of the sternum, affording protection to large, easily injured abdominal organs such as the liver, spleen, stomach, and kidneys.
The thoracic and abdominal cavities are separated by the dome-shaped diaphragm, a sheet of tissue consisting of a peripheral muscular part and a central tendinous part that closes the thoracic cavity interiorly. Superiorly, the narrow upper thoracic aperture—bounded by the upper part of the sternum, the short stout first ribs, and the body of the first thoracic vertebra (T1)—gives access to the root of the neck and is not closed by a specific structure. The thorax is bounded posteriorly by the bodies of the 12 thoracic vertebrae and the posterior portions of the ribs, anteriorly by the sternum, costal cartilages, and anterior portions of the ribs, and laterally by the remaining parts of the ribs. The spaces between successive ribs are bridged by the intercostal muscles.
The sternum (breastbone) lies anterior in the midline and superficially. The clavicles and the first seven pairs of ribs articulate with it. The sternum consists of three parts: the bony manubrium and corpus sterni and the small, cartilaginous xiphoid process. The clavicles articulate with the manubrium on its upper border, and the notch between these joints is the interclavicular (or suprasternal) notch. Just below the sternoclavicular joints, the cartilages of the first ribs are attached to the sternum. No joint spaces are present here. The manubrium and the body of the sternum are united by fibrocartilage. The junction between the manubrium and the body of the sternum usually forms a prominent ridge, accentuated by the two parts of the sternum forming a slight angle with each other, the sternal angle of Louis. This is an important landmark because the cartilages of the second ribs articulate with the sternum at this point. The third, smallest part of the sternum is the xiphoid cartilage, a thin, spoon-shaped process attached to the lower end of the sternal body.
Most of the bony thorax is formed by the ribs, usually 12 on each side of the trunk. The ribs consist of a series of thin, curved, rather elastic bones that articulate posteriorly with the thoracic vertebrae and terminate anteriorly in the costal cartilages. The first seven pairs of ribs attach to the sternum by means of their cartilages, whereas the eighth, ninth, and tenth pairs articulate with each other and do not reach the sternum. The 11th and 12th pairs are small and poorly developed, ending in free cartilaginous tips. The ribs are thickest posteriorly; they flatten out and widen as they curve forward. Along the inferior and inner surface of the posterior part of each rib, a groove—the sulcus costae—affords protection to the intercostal vessels and nerve.
The first two and last two ribs differ somewhat from the previous description. The first rib (see Plate 1-2) is very short and relatively heavier than the other ribs. On the superior surface of the first rib, two grooves are divided by a tubercle—the tuberculum scaleni—that forms the point of insertion of the anterior scalene muscle. The groove in front of the muscle is occupied by the subclavian vein, whereas the subclavian artery follows the groove behind the tubercle. The second rib is longer than the first and resembles the other ribs except the small 11th and 12th ribs.
The spaces between successive ribs are occupied by intercostal muscles (see Plate 1-1). Each external intercostal muscle arises from the lower border of the rib above, runs obliquely downward and medially, and inserts into the upper border of the rib below. Each internal intercostal muscle arises from the lower border of the rib above and runs downward and outward to insert on the upper border of the rib below. Between these two muscle layers lie the intercostal vessels, whereas the intercostal nerves lie between the internal and the innermost intercostal muscles.
Many muscles of the upper extremities originate from the chest wall, including the pectoralis major (see Plate 1-1) and pectoralis minor muscles and the serratus anterior muscle, which originate from the anterior and lateral portions of the chest wall.
Several neck muscles originate from the upper rim of the thoracic cage. The sternohyoid and sternothyroid (see Plate 1-1) are thin, straplike muscles that arise from the superior border and posterior surface of the sternum and insert into the hyoid bone and the thyroid cartilage, respectively. The sternocleidomastoid muscle (SCM) arises (see Plate 1-1) as a stout sternal head from the upper border of the sternum, adjacent to the sternoclavicular joint, and as a second clavicular head from the medial third of the clavicle. The interval between the two heads is usually visible as a slight depression, behind which the apex of the lung rises from the thorax into the root of the neck. Above this interval the two heads of the SCM unite to form a single muscular belly that passes obliquely upward, backward, and laterally to insert into the lateral surface of the mastoid process and occipital bone.
Superficial to the SCM, the external jugular vein passes perpendicularly downward from its origin at the lower border of the parotid gland, crosses the SCM, and penetrates the deep fascia of the neck to empty into the subclavian vein.
Of the deeper neck muscles, the three scalene muscles originate from the transverse processes of the cervical vertebrae. The anterior scalene muscle inserts into the scalene tubercle of the first rib; the medial scalene muscle also attaches to the upper surface of the first rib, but more posteriorly. The posterior scalene muscle inserts on the second rib. The components of the cervical nerve plexus emerge from the groove between the anterior and middle scalene muscles. The anterior scalene muscle is crossed laterally and anteriorly by the phrenic nerve, which originates from the cervical plexus and runs downward and behind the subclavian vein to enter the thoracic cavity. The groove between the anterior and middle scalene muscles widens inferiorly to form a triangular opening through which emerge the components of the brachial plexus and the subclavian artery. After ascending from the thoracic cavity, the subclavian artery crosses the upper surface of the first rib, lying in the groove posterior to the scalene muscle, and enters the axilla. The subclavian vein runs parallel to the subclavian artery but in front of the anterior scalene muscle.
Deep in the lower portion of the neck under the SCM, a narrow space is bordered anteriorly by the omohyoid and strap muscles, posteriorly by the anterior scalene muscle and prevertebral fascia, and medially by the pharynx, esophagus, trachea, and thyroid gland (see Plate 1-1). In this space the common carotid artery, internal jugular vein, and vagus nerve are enclosed in a common connective-tissue sheath; the jugular vein runs most superficially and the vagus nerve lies beneath, between the common carotid artery and internal jugular veins. On the left side the thoracic duct (see Plate 1-1) crosses over the subclavian artery and runs anteriorly to empty into the proximal subclavian vein.
Blood for the chest wall is supplied by the intercostal arteries and the internal thoracic (internal mammary) arteries. After originating from the aorta, the posterior intercostal arteries cross the vertebral bodies and enter their corresponding intercostal spaces, passing along the inferior border of the ribs between the internal and external intercostal muscles. The vessels are well protected posteriorly by the subcostal groove. The internal thoracic arteries originate from the inferior surface of the subclavian arteries and run downward, lateral to, and (for a short distance) with the phrenic nerve, reaching the posterior surface of the anterior chest wall. The arteries continue their downward course for approximately  inch laterally to the edges of the sternum, dividing just above the diaphragm into their two terminal branches: the musculophrenic and superior epigastric arteries. Along their course the internal thoracic arteries give rise to branches to the thymus, mediastinum, and pericardium posteriorly; to the perforating branches to the skin and subcutaneous tissues anteriorly; and finally to the lateral branches that pass along the rib cartilages and anastomose with the posterior intercostal arteries.
inch laterally to the edges of the sternum, dividing just above the diaphragm into their two terminal branches: the musculophrenic and superior epigastric arteries. Along their course the internal thoracic arteries give rise to branches to the thymus, mediastinum, and pericardium posteriorly; to the perforating branches to the skin and subcutaneous tissues anteriorly; and finally to the lateral branches that pass along the rib cartilages and anastomose with the posterior intercostal arteries.
The veins of the thoracic wall correspond in their course with the arteries. The 10 lower intercostal veins on the right enter the azygos vein, and the upper two intercostal veins enter either the azygos or the brachiocephalic (innominate) vein. The lower intercostal veins on the left side enter the hemiazygos or accessory hemiazygos vein. The three left superior intercostal veins enter the left brachiocephalic vein by a common stem, the left superior intercostal vein.
The chest wall receives its nerve supply from the intercostal nerves, which accompany the intercostal vessels.
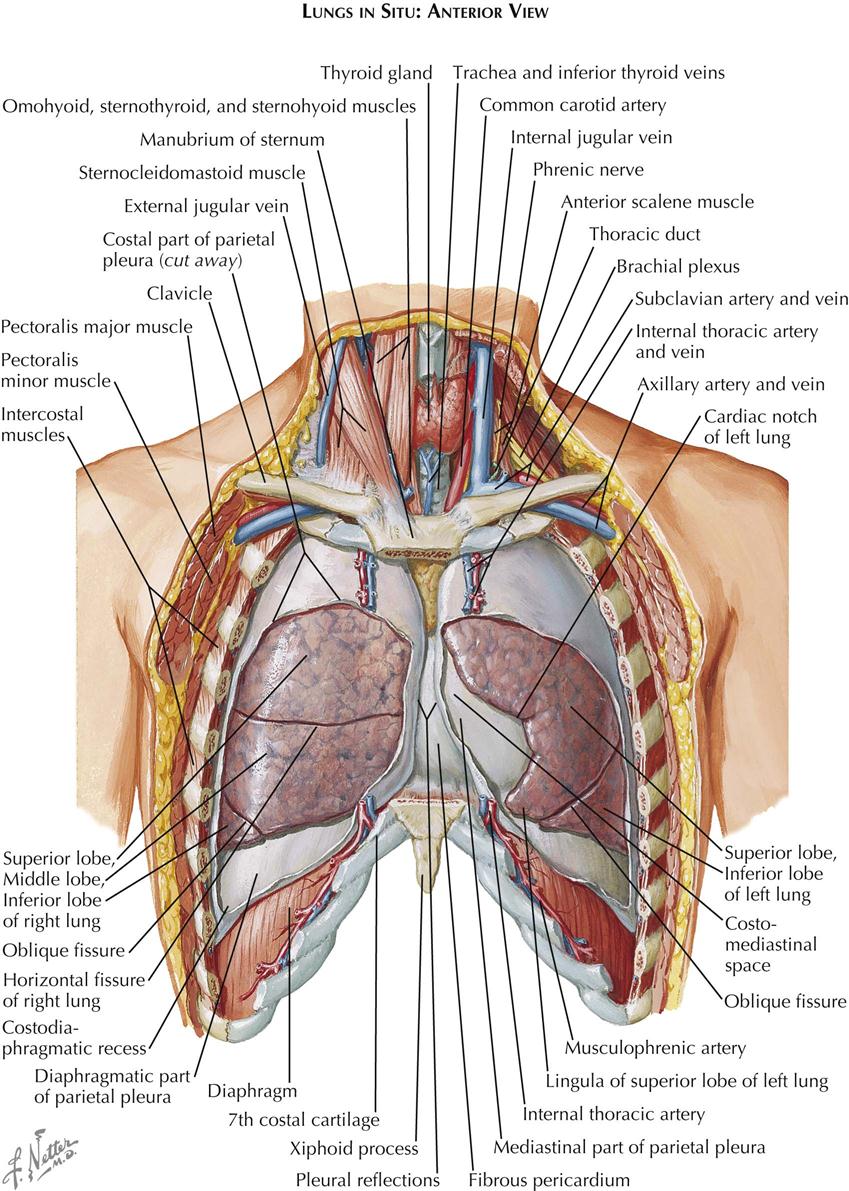
Most of the thoracic cavity is occupied by the two lungs, each of which is enclosed by its pleura. Each pleura forms a closed sac invaginated by the lung so that part of it covers (and is adherent to) the inner surface of the chest wall, the diaphragm, and the mediastinum, known as the costal, the diaphragmatic, and the mediastinal pleura, respectively, and collectively as the parietal pleura (see Plate 1-2). That part of the mediastinal pleura that covers the pericardium is called the pericardial pleura; the remainder (visceral pleura) covers the lung. The virtual space between the visceral and parietal pleurae contains a tiny amount of clear fluid. The pleural reflections (see Plate 1-1), between the costal and diaphragmatic portions of the parietal pleura, lie lower than the corresponding lower edge of the lung. The resulting space normally is not completely filled by the lung, even on deep inspiration, and is called the recessus costodiaphragmaticus.
The right lung consists of three lobes—the superior, middle, and inferior lobes—and is somewhat larger than the left lung, which has two—the superior and inferior lobes (see Plate 1-1). The smaller size of the left lung results from the eccentric position of the heart, which encroaches on the left pleural cavity. The two pleural cavities almost meet behind the upper sternum, but the left costomediastinal reflection deviates laterally below the fourth rib cartilage, exposing a small triangular portion of the pericardium that is not covered by pleura. At the same level, the anteroinferior portion of the left superior lobe recedes even more, leaving a portion of the pericardial pleura that is not covered by lung tissue.
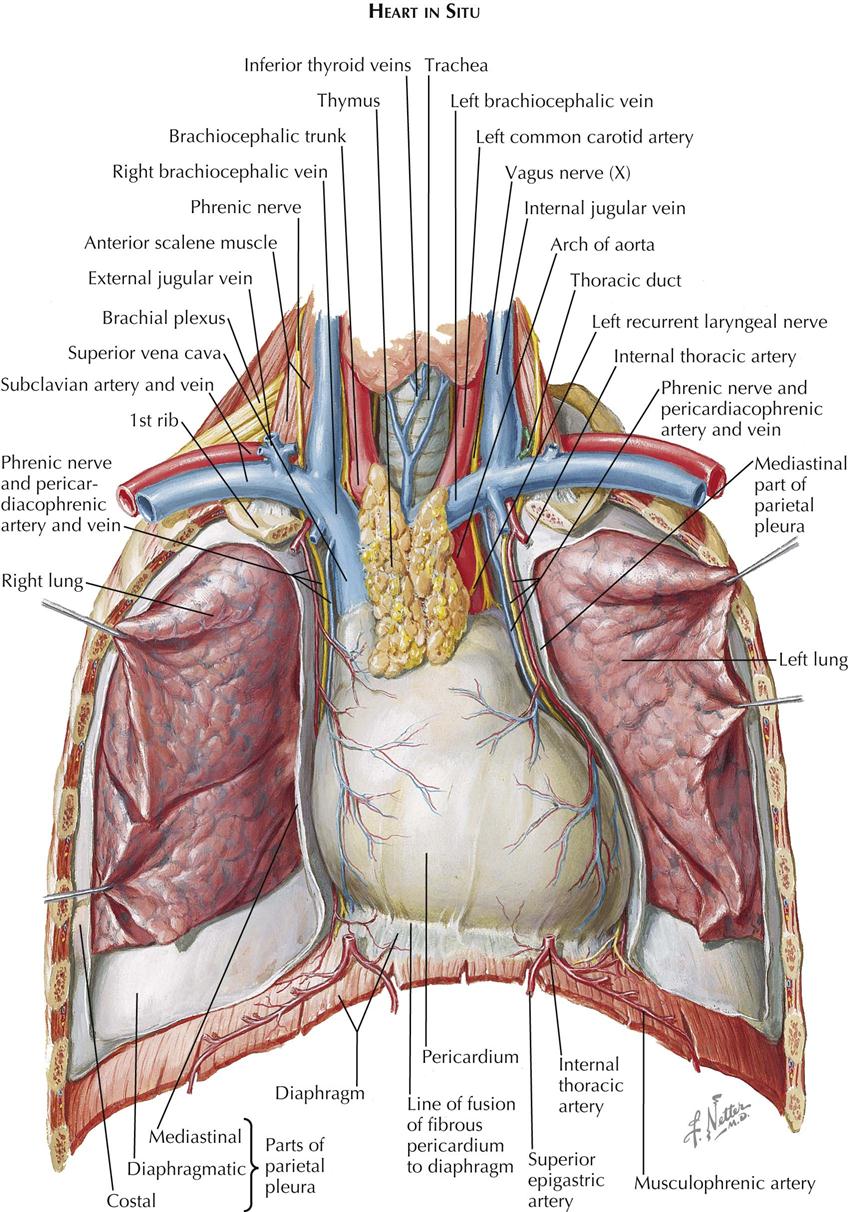
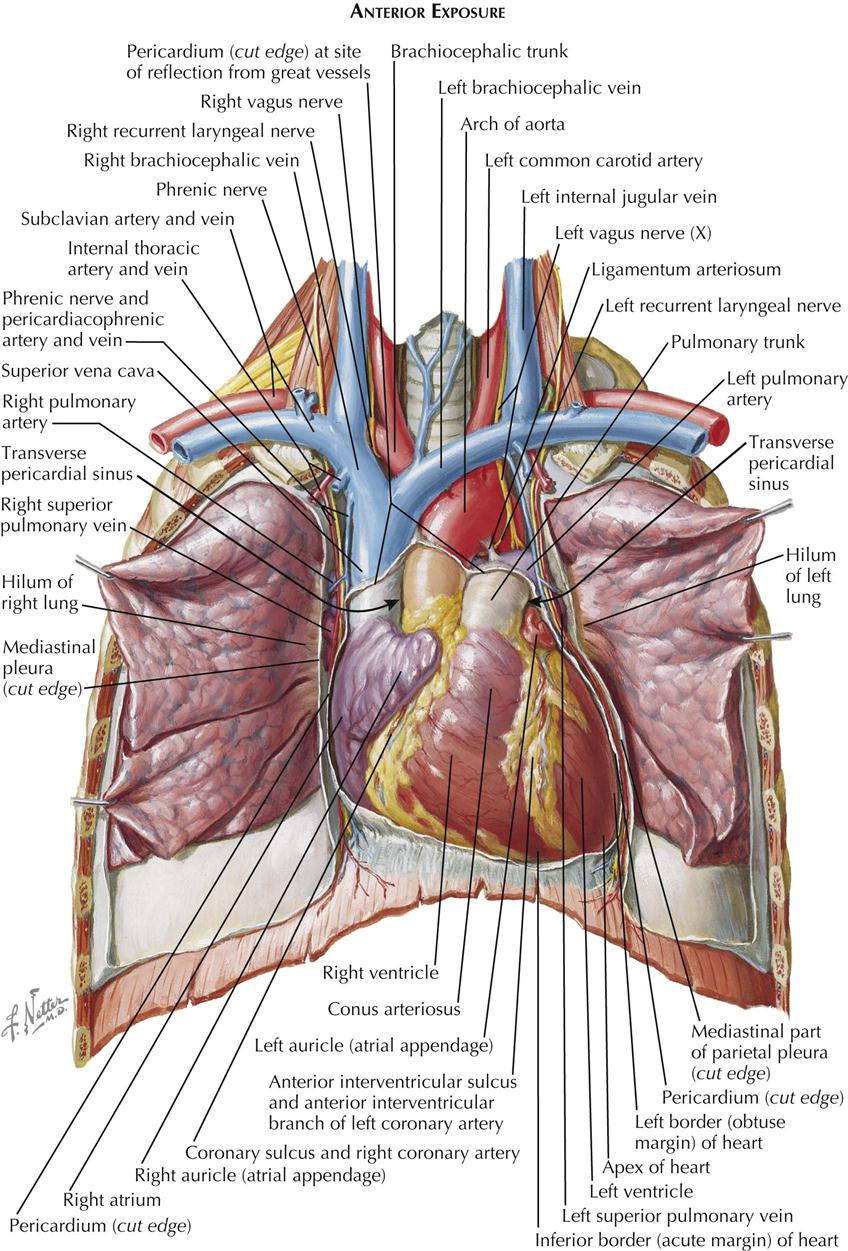
The central space between the two pleural cavities is the mediastinum. The mediastinum is divided arbitrarily into superior, anterior, middle, and posterior mediastina. The shallow anterior mediastinum contains a portion of the left internal thoracic vessels and the vestigial transverse thoracic muscle. The superior mediastinum contains the thymus gland (see Plate 1-2), which largely disappears by about age 12 years leaving a small pad of fat and areolar tissue, and the brachiocephalic veins, which join each other on the right to form the superior vena cava (see Plate 1-5). Posterior to the brachiocephalic veins, the phrenic and vagus nerves descend from the neck. The phrenic nerves, accompanied by the pericardiacophrenic vessels, run laterally, anterior to the lung roots and along the pericardium, until they reach the diaphragm.
The aortic arch ascends from the heart into the superior mediastinum, almost reaches the upper border of the manubrium sterni, courses obliquely backward and to the left over the left main bronchus, and continues as the descending aorta downward, anteriorly, and slightly to the left of the vertebral column. Originating from the convexity of the arch, from the proximal to the distal position, are the brachiocephalic, left common carotid, and subclavian arteries.
The right vagus nerve (see Plate 1-5) passes between the subclavian artery and vein and gives off the right recurrent nerve, which loops around the subclavian artery to ascend along the trachea. The left vagus nerve runs between the subclavian vein and the aortic arch, giving rise to the left recurrent nerve (see Plate 1-5), which similarly loops around the arch to ascend along the trachea.
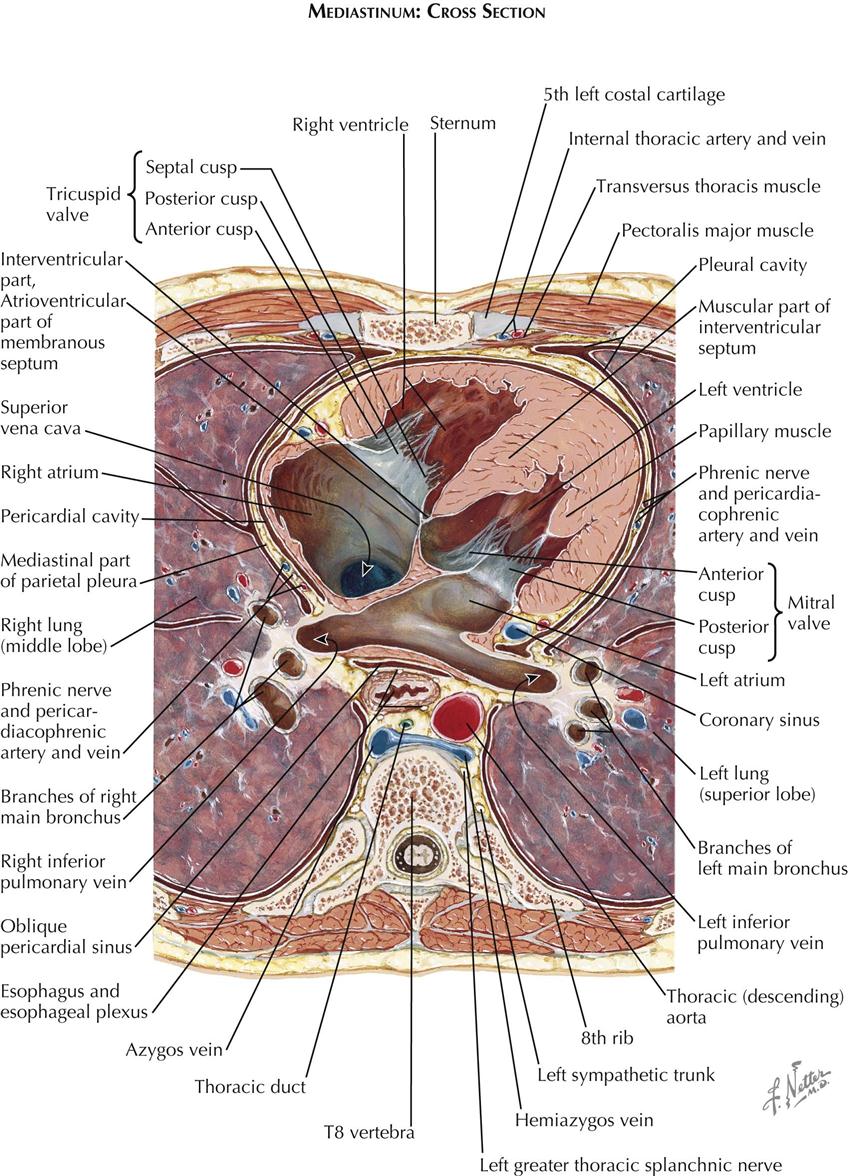
The trachea descends from the neck behind the aortic arch and bifurcates into right and left main bronchi at the level of the sternal angle. Behind the trachea runs the normally collapsed esophagus (see Plate 1-4), joined by the vagus nerves just beyond the branching off of the recurrent nerves from the vagi. Behind the esophagus, between the azygos vein and the descending aorta, the thoracic duct (see Plate 1-2) ascends, coursing behind the aortic arch to enter the neck, where it empties into the left subclavian vein.
Against the necks of the ribs, the sympathetic trunks descend from the neck, first giving off the greater thoracic splanchnic nerve (major splanchnic nerve) (see Plate 1-3) at about the level of the sixth rib and then the minor or lesser and lowest thoracic splanchnic nerves.
The posterior mediastinum is a shallow space containing the lower portions of the esophagus, vagus nerves, descending aorta, azygos and hemiazygos veins, thoracic duct, and sympathetic nerve chains. The remaining and largest part of the mediastinum, the middle mediastinum, contains the pericardium, heart, lung roots, and phrenic nerves.
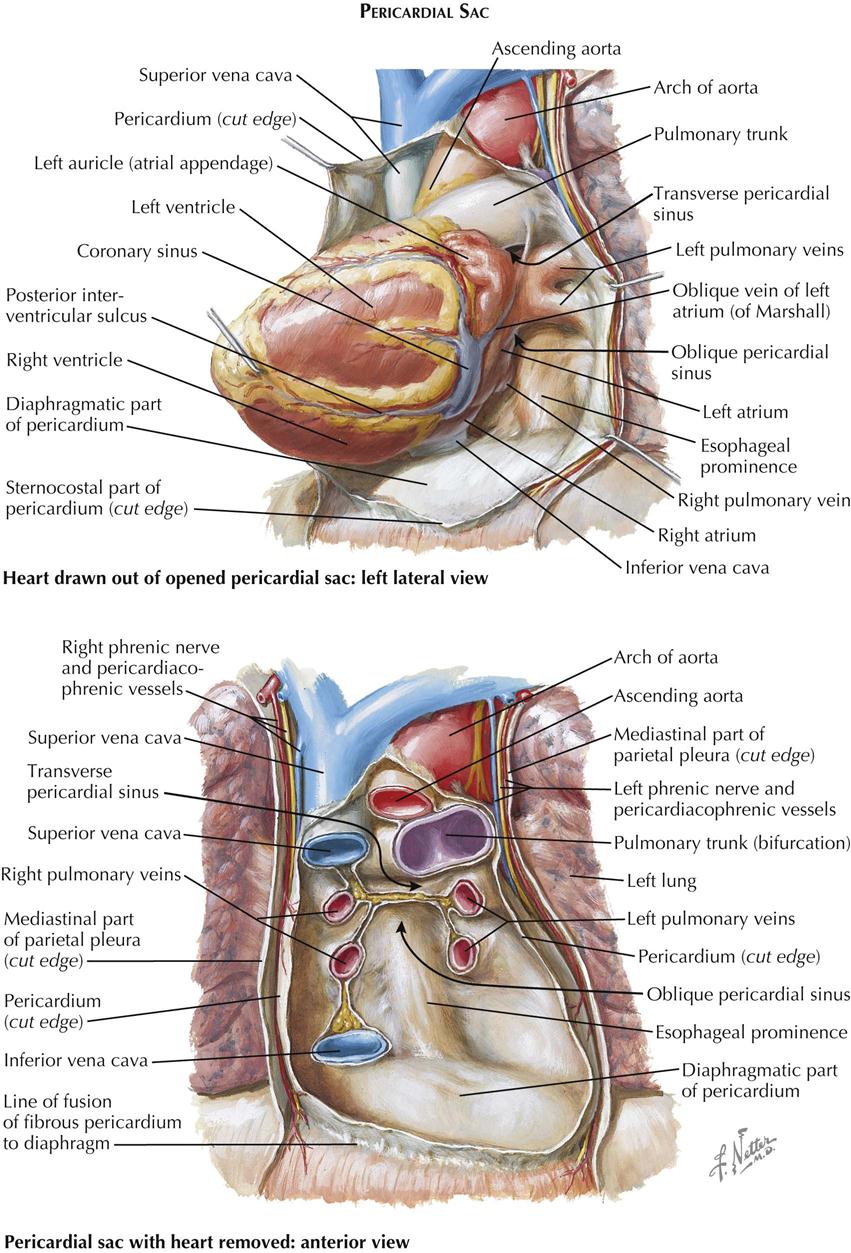
The pericardial cavity is the third serous cavity contained in the chest, with the two pleural cavities. The pericardial cavity is conical in shape, with the base of the cone lying posteriorly to the right and the apex anteriorly to the left. It completely invests the heart and the proximal portions of the great vessels. As with the pleura, a visceral portion of the pericardium is distinguished overlying the heart and proximal great vessels, usually called the epicardium, as is a parietal portion. The inferior part of the parietal pericardium is densely adherent to the middle tendinous part of the diaphragm. Most of the lateral and anterior portions are contiguous but not normally adherent to the pleura. A small triangular part of the anterior portion of the parietal pericardium lies directly behind the sternum, separated only by areolar and fatty tissue (endothoracic fascia) and the transverse thoracic muscle.
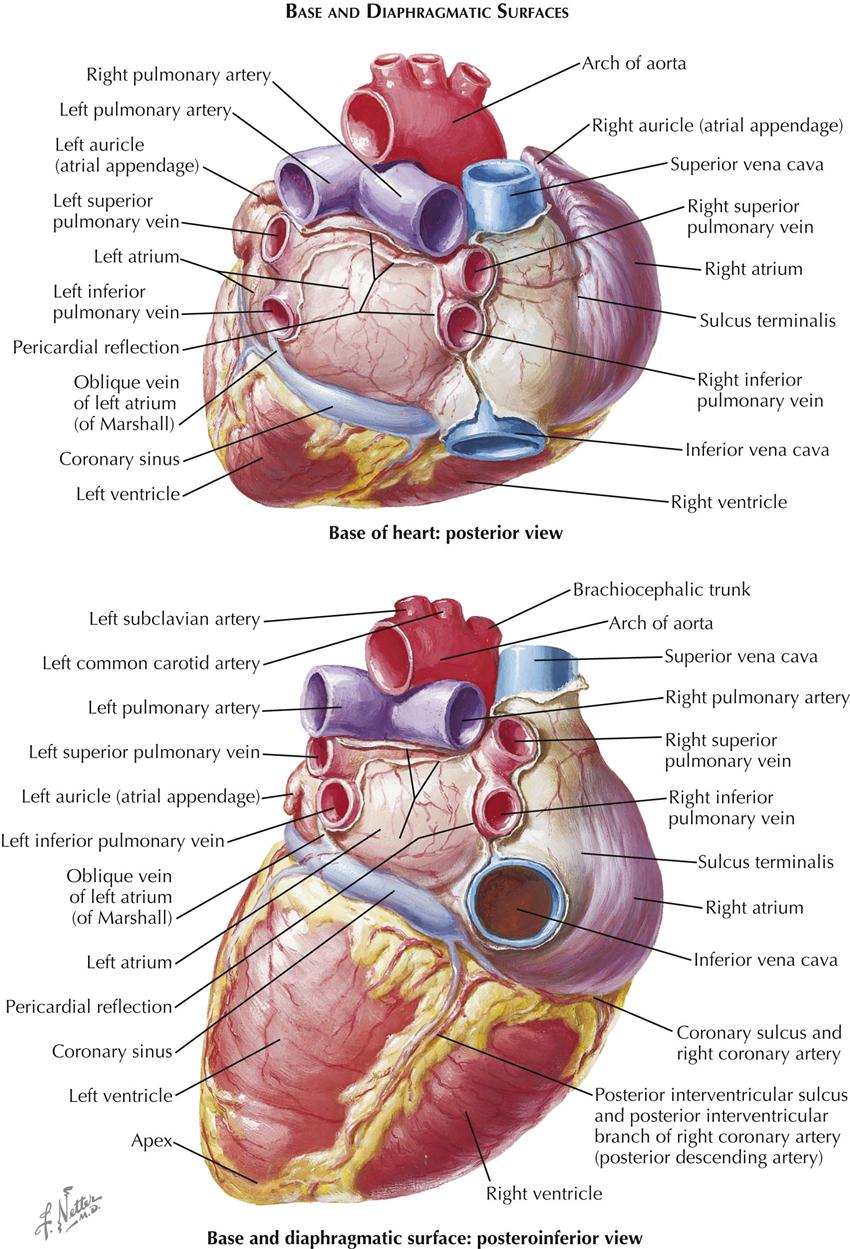
The great vessels enter and leave the pericardial cavity at its base. A curved, transversely running passageway between the arterial and venous poles of the heart is called the transverse pericardial sinus. Posteriorly, a blind recess of the pericardial cavity is bordered by the pericardial reflection between the pulmonary veins and inferior vena cava, called the oblique pericardial sinus. Small recesses exist between the superior and inferior pulmonary veins on each side and behind the fold of the left vena cava (ligament of Marshall), a small crease of pericardium running from the left aspect of the pulmonary trunk to the left atrium, between the neck of the left auricle and the left pulmonary veins. The left vena cava fold contains the vestigial remains of the left common cardinal vein.
Exposure of the Heart
Sternocostal Aspect
Within the pericardium lies the heart, a hollow, muscular, four-chambered organ suspended at its base by the great vessels. In situ the heart occupies an asymmetric position, with its apex pointing anteriorly, inferiorly, and about 60 degrees toward the left. Its four chambers are arranged in two functionally similar pairs, separated from each other by the cardiac septum (see Plate 1-5). Each pair consists of a thin-walled atrium and a thicker-walled ventricle.
The anatomic nomenclature of the heart removes it from the body and places it on its apex, and thus the cardiac septum is in a sagittal plane. This practice has led to misconceptions and difficulties in orientation among cardiologists and surgeons. On a chest radiograph, for example, the left cardiac border is formed by the left ventricle, but the right border is formed by the right atrium, not the right ventricle, which lies anterior. The major and important part of the left atrium lies directly posterior and in the midline in front of the spine and esophagus, allowing the pulmonary veins to be as short as possible.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


